We would like to welcome you to our Open Day at the DLT warehouse, offices and showrooms in Huddersfield.
Free entry and open to all with special offers and discounts on the day. Our famous Yorkshire hospitality will be on display with plenty of food and drink for you to enjoy.
• 10% Discounts on the day
• Deals on equipment
• Want to view a particular product?
Email JulianBall@dltchiropody.co.uk and he will arrange this for you.
The day will run from 10am to 4pm on Saturday 8th June. We are running two workshops:
• An introduction to using Radial Extracorporeal Shockwave Therapy which is a safe and effective treatment for chronic muscle and tendon pain. Times 11am – 12pm & 1pm – 2pm.
• Heat Moulding ICB Orthotics – ICB Orthotics are very versatile and can be custom fitted by heat moulding to the patients foot.
Times 10am – 11am & 12pm – 1pm.
To guarantee a place please use the booking form here but there will be many spaces on the day.
A Dorsiflexed 1st Ray (Metatarsal) also known as metatarsus Primus describes a deformity in which the 1st Ray /Metatarsal lies in a dorsiflex position relative to the lesser metatarsals.
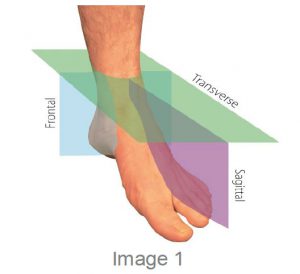
The first ray is made up from the first metatarsal and the medial cuneiform. The ray facilitates movement in all three planes however predominantly produces the frontal and sagittal plane movements of dorsiflexion coupled with inversion and plantarflexion with eversion. This is due to its axis being 45° to both of these planes.
The biomechanics of this condition and the compensatory mechanisms and the resultant limitations need to be considered to understand both the function issues and the possible treatment that will need to be proposed for this condition.
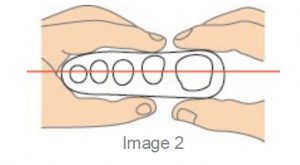
The first ray (metatarsal) normally sits parallel to the plane of the lesser rays with equal amounts of dorsiflexion and plantarflexion usually 5mm up and 5mm down to allow the required plantarflexion to enable 65° to 75 °of MPJ dorsiflexion during the propulsive phase.
A Dorsiflexed 1st Ray is an osseus deformity where the lesser metatarsals sits lower to the bisection of the 1st Metatarsal when the foot is in the STJN position.
The condition may be congenital or acquired and is often referred to as ‘metatarsus primus elevatus’ or simply the prime metatarsal is elevated in reference to the lesser.
It should not be confused with Forefoot Supinatus as once the foot is placed in STJN the shaft can, with a supinatus, be plantarflexed. However, we should understand that the dorsiflexed 1st can be both fixed and or mobile in nature.
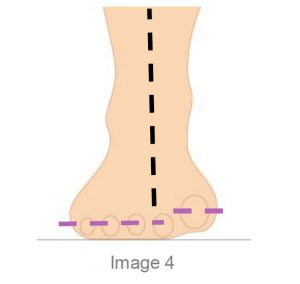
Because the 1st metatarsal is dorsiflexed it encourages the foot to collapse medially inhibiting the phalange from propelling over the 1st MTPJ, jamming occurs and a reduction in the ROM of the joint may be experienced.
The result of this jamming will be a stiffening of the joint and often the patient will develop an adductory twist in gait to reduce the load on the 1stMTPJ, as this occurs callosity will develop on the medial aspect of the hallux.
The distal phalanx of the hallux can also be forced into dorsiflexion as a toe off compensation, causing a hole to wear on top of the shoe and thickening of the nail from the constant trauma on the dorsal toe.
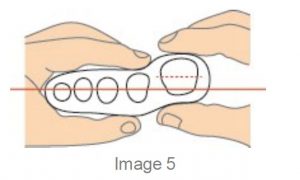
Clinical assessment of Metatarsal Phalangea Elevatus ( MPE) involves the evaluation of the sagittal plane position of the joint. The patient is evaluated in a non-weight bearing supine position with the subtalar joint in its neutral position (use the ICB AAM method) for Neutral.
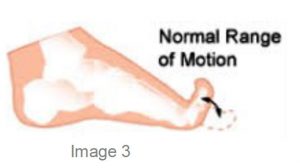
As previously stated Metatarsus primus elevatus can be described as being congenital or acquired and can be further classified as a rigid, semi rigid, mobile or hypermobile deformity. A normal range of motion usually indicates a congenital deformity whilst an acquired.
MPE is characterised by an abnormal range of motion. This may be due to tibialis anterior contracture or associated with a forefoot supinatus.
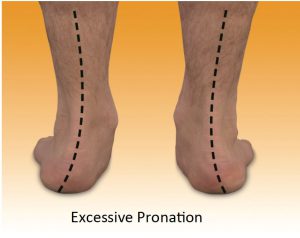
The main issue is that the elevated metatarsal encour-ages the foot to function similar to a forefoot varus and excessive pronation is a key element as the foot collapses medially to allow normal ground contact in the toe off phase. Treatment will be a Morton’s ramp extension.
The purpose of the treatment is to allow a more normal ‘toe off’ to occur in the gait cycle by filling the gap under the 1st MTPJ whilst supporting the proximal hallux and thereby allowing earlier loading to occur.
To create the Mortons ramp to lift the proximal hallux this can be achieved by using a ICB 4° Forefoot addition (acts like a Morton’s ramp Image 9) to support the hallux and allow it to propel over the 1st metatarsal joint during toe off stage of gait.
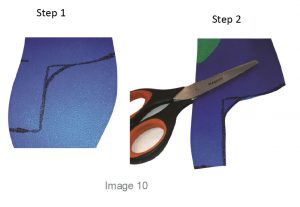
A Full Length orthotic can also be used to create a Morton’s extension, use the forefoot addition to provide the required lift. See image 10 add the addition and mould to the foot in Neutral. First mark out the Morton’s extension ramp shape , cut and use a hand grinder to smooth the distal edges.
Orthotic therapy is not an exact science, so be prepared to adjust the orthotic for the patient by adding or subtracting as needed.
General REFERENCES
1. Merriman, L.M. and Tollafield, D.R. (1995) Assessment of the Lower Limb. Churchill Livingstone, Singapore Figure 2: Evaluation of first ray position(Merriman and Tollafield, 1995)
2. Root M L, Orien W P, Weed J H., 1977 Normal and Abnormal Function of the Foot. Clinical Biomechanics Vol 2, Los Angeles
3.Merriman’s assessment of the Lower Limb 3rd Ed. Churchill Livingstone
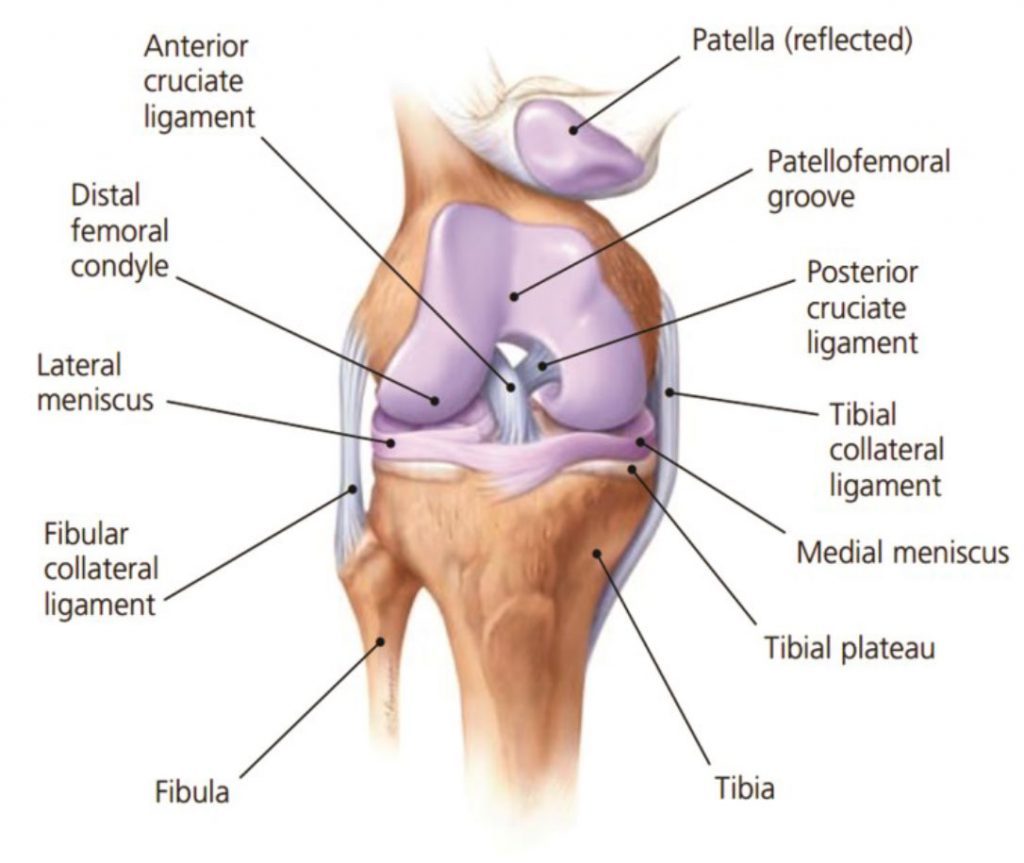
The knee joint is the largest joint in the human body consisting of two articulations: one between the femur and tibia, and one between the femur and patella. It is commonly described as a ‘hinge joint’, being a combination of a hinge and pivot-joint, which permits flexion and extension as well as a slight internal and external rotation.
The knee joint consists of an articulation between four bones: the femur, tibia, fibula and patella, and comprises of four compartments. These are the medial and lateral tibiofemoral compartments, the patellofemoral compartment and the superior tibiofibular joint. The components of each of these compartments can suffer from repetitive strain, injury or disease.
There are many reasons for experiencing knee pain such as, sprained ligaments, meniscus (cartilage) tears, tendonitis, and excessive supination and excessive pronation. The knee is a complex joint, and it can experience pain due to an exaggerated Q angle of the upper leg, for example.
Some of the conditions that can affect the anterior knee compartment are conditions such as :
Patellofemoral pain syndrome
Chondromalacia Patella
Osgood-Schlatter’s disease
Sinding Larsen Johansson syndrome
Knee bursitis/Hoffa’s disease
Generally in this article we will be dealing with non-trauma induced pain or biomechanically induced pain which is often described as idiopathic in nature.
Often when the subject is discussed terms such as ‘Retro Patella pain’, ‘Patella Femoral Dysfunction’, ‘Medial Compartment Syndrome’, ‘Chondromalacia Patella’ or ‘Iliotibial Band Friction Syndrome’ – these conditions are descriptions of knee pain (or pain centres) and do not indicate causative factor/s contributing to the experience of the pain.
Generally pain can be experienced Medial, Lateral or Anterior aspects and it is recommended that the Symptomatic treatment approach is adopted which, treats the pain and then progressively treats the underlying causative factors.
Understanding the dynamics of the knee joint is important in understanding why certain foot mechanic issues can impact upon the knee compartment. The knee is one of the most important joints in our body, playing an essential role in movement related to carrying the body weight horizontally (in running and walking) and in a vertical direction (jumping and absorbing ground reaction impact). The ligaments surrounding the knee joint offer stability by limiting medial and lateral movements, and together with several menisci and bursae, protect the articular capsule.
There is an allowance in the knee joint for a small amount of medial and lateral movement of between 3°-5°. Movement in excess of this puts the patient at risk of experiencing medial collateral ligament and lateral collateral ligament damage.
Both excess pronation and excess supination can have a deleterious effect on the medial and lateral collateral ligaments as outlined by Michaud 1 in which he states that for every 1˚ of pronation and or supination, the tibia internally or externally rotates 1˚, which in turn impacts on the knee joint, as it bears the stress generated by the tibial rotation.
When both excessive internal and excessive external rotation are experienced together excessive movement of the patella ligament occurs and pain can be experienced anteriorly.
Tiberio(2) notes that malalignment factors such as, excessive rotation of the lower leg which accompanies subtalar joint pronation has been cited as a major contributor to patellofemoral dysfunction.
There appears to be a direct link to knee pain from foot mechanics issues and therefore identifying and treating basic lower limb biomechanics appears to have a beneficial affect for patients.
Controlling both pronation and addressing any issues with forefoot will be a determining factor in addressing anterior knee pain.
The medial collateral ligament (MCL) connects the femur to the tibia, whilst the lateral collateral ligament (LCL) connects the femur to the fibula and both work to stabilise the knee by bracing and protecting the sideways movement.
The lateral collateral ligament is placed under stress by lateral biomechanical factors such as supination, internal lateral rotation of the tibial shaft and the impact of an untreated forefoot valgus deformity.
Patients that present with a high forefoot valgus FFTVL in excess of 10° will supinate their foot from heel strike to toe off which will stress the lateral knee compartment.
Excessive pronation will cause internal tibial rotation producing stress on the medial collateral ligament.
Idiopathic anterior knee pain however, is often results from a combination of both pronation and supination in which the anterior patella attachment is aggravated by the Lateral to medial movement in the gait cycle.
A Forefoot Valgus less that 10° will allow the patient to heel strike lateral, the ground ‘reaction forces’ are sufficient to propel the foot into pronation at mid stance to toe off due to the lower Forefoot valgus deformity.
The movement at mid stance, in this situation, is rapid and as the supination to pronation movement occurs the patella tendon moves lateral to medial placing additional stress on the tendon.
Stabilising the foundation and reducing excessive movement around the sub talar joint ( STJ) is essential, a reduction in tibial rotation will have beneficial effects on collateral stress at the knee compartment.
A key point in the orthotic therapy to treat knee pain is that the orthotic is correctly fitted and aligned to the bisection of the calcaneus and the alignment of the tibia or tibial varum angle. Failure to adequately address this issue will result in the patient continuing to exhibit the same foundational instability or allow the patient to, in the case of pronation, to ‘collapse the arch onto the orthotic’ due to the poor rearfoot correction.