![]()
Often practitioners ask if there is really any reason that they should bother heating and moulding the ICB orthotic product.
Whilst the product can be used directly out of the presentation pack and placed into the shoe, heat moulding provides an added dimension in maximising patient compliance.

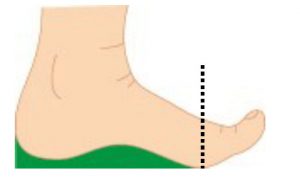
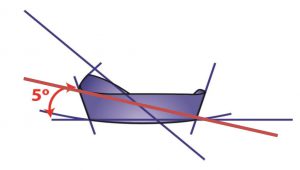
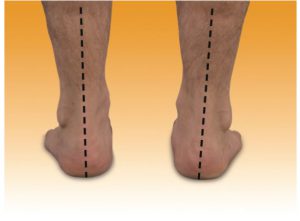
Generally we recommend that upon observation if the rearfoot position is lower than +3° or greater than +6° heat moulding will definitely benefit the patient. The ICB product exhibits a 5° rearfoot varus Intrinsic angle to assist in realignment of the calcaneus.
When treating rearfoot greater than 5° – 6° will be beneficial and for more pes planus foot types reducing the average 42° arch height will provide more comfort for the patient.
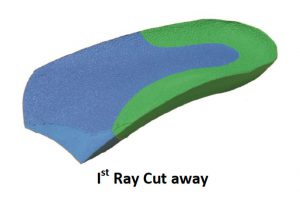
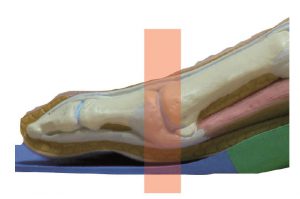
When a deflection is required to deflect around a callus etc. practitioners can use a spoon to make a deflection directly in the product.

Often practitioners have to deal with highly unusual foot issues and the use of an adaptable heat mouldable product can be extremely helpful. Product should be chosen with the mindset that they have the capability to be modified and when the situation arises they then have the tools to perform that particular function for the patient.

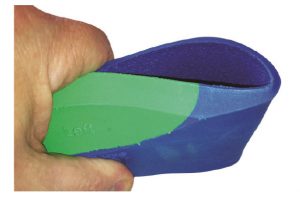
The moulding above may seem extreme , however this product was actually customised for a patient in Asia.
The patient suffered an injury and the foot was set in a particular position which created a functional right long leg.

The patient refused further surgery and requested conservative treatment. This extreme moulding was combined with shoe wear that had a large heel height such as a boot to provide the desired result for the patient.
Practitioners are encouraged to experiment and use alternate methods of moulding to the patients foot shape. One such method is pictured, the foot and orthotic is wrapped in a bandage in the ideal or STJN position due to the patients inability to weight bear.

Difficulty can be experience when treating children and so alternate moulding methods should be experimented with in an endeavour to be able to treat the entire patient base.
Issues with treating children and heat moulding can be overcome by using a non weight bearing moulding method as seen below.

This non weight bearing method can be very effective. The use of the Anterior Alignment Method for ideal or STJN is recommended to establish positioning.
The ICB normal method of moulding is in weight bearing position, however, alternate methods can be used to treat patients whilst maintaining the patients ideal position.
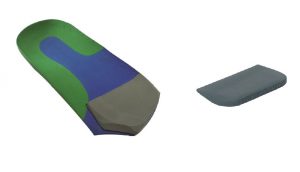
Generally product that does NOT have a material cover can be heated on the dorsal and plantar surface, whereas with covered product such as, seen below , should only be heated on the plantar surface to avoid burning the material cover.

A recent development in the ICB product is the reduction in the heat time that is required to attain the optimum level of elasticity in the EVA material.
Close observation to the heating process is necessary to produce a well moulded product. Re-moulding is possible with the ICB Heat mouldable product, albeit with some loss of density integrity in which 5-7% softening of the molecular structure will be experienced on the re-heating of the product.
To start maintain the heat gun at a distance of approx. 10-15cm. The heating process commences by using 3 circular motions on the plantar surface located in the medial arch area concentrating on the words RIGHT & LEFT and then a further circular motion on the plantar heel area.
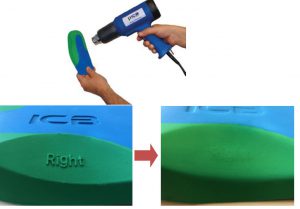
Continue until the words RIGHT and LEFT tart to Melt indicating that the thermal heat level has been attained.
Request that the patient inserts the UN HEATED product in their shoe as this will provide foundational stability and avoid causing a functional leg length.
Next remove any factory fitted shoe innersole and place the heated product in the shoe.

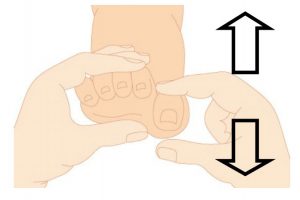
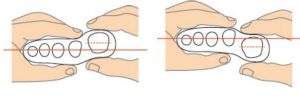
Place the foot to be moulded in the ideal or neutral position using the Anterior Alignment method and Talo Navicular method.
Maintain for 30-40 seconds. Then remove the product and allow to cool down approx. 1-2 minutes and commence the procedure again for the alternate foot.