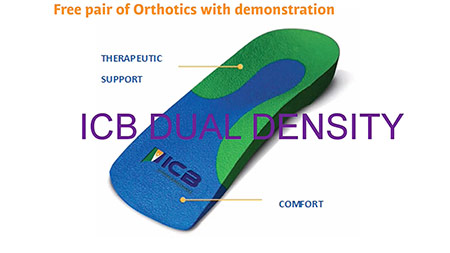
I would like to arrange an ICB Orthotic demonstration at my clinic and claim my free pair of ICB Orthotics.
The demonstration will include heat moulding and how to place the foot into the neutral position and take no longer than 30 minutes.


I would like to arrange an ICB Orthotic demonstration at my clinic and claim my free pair of ICB Orthotics.
The demonstration will include heat moulding and how to place the foot into the neutral position and take no longer than 30 minutes.
This course will present a foundational understanding of lower limb biomechanics by independent pre-learning together with a workshop on practical orthotic therapy. Taught by Lawrence Dreifuss owner of Tuckton Chiropody & Podiatry Centre.

PRACTICAL HANDS ON WORKSHOP OBJECTIVES:
This practical ‘hands on’ day will provide the manual skills to implement chairside orthotic therapy to fulfil a successful treatment plan for your patient.
Upon completion of this workshop, the participants will be able to:
▪ Identify Neutral Calcaneal Stance Position (NCSP)
▪ Assess for Structural Leg Length Discrepancy
▪ Heat and moulding orthotics to the patient’s STJN
Evaluate and treat forefoot mechanics, including:
▪ Forefoot Valgus
▪ Forefoot Varus
▪ Plantarflexed 1st
▪ Dorsiflexed 1st
Perform chairside orthotic modifications, including:
▪ Plantar fascial grove to treat tight Fascia
▪ Extrinsic and Intrinsic metatarsal Dome for Metatarsalgia and Mortons Neuroma
▪ 1st Metatarsal deflection to treat plantarflexed 1st
▪ Forefoot Varus and Forefoot Valgus posting
▪ Morton’s extension for HAV, Dorsiflexed 1st & Hallux limitus.
Attendees will receive a starter pack (worth over £100) which will include a pair of orthotics to heat mould, plus a set of products to deflect and customise in the workshop.
We provide prior learning 30 days before the course, to ensure all participants benefit from the subjects taught on the day.
Dates are:
OR CONTACT RICHARD ON 07553 345 831OR EMAIL richard@dltpodiatry.co.uk
 |
FULL !! FULL!!! SUNDAY 4TH MARCH AT DLT PODIATRY SUPPLIES – HUDDERSFIELD- HD1 4TW |
OPEN DAYFree entry and open to all, special offers and discounts available on the day. We bring our showroom to you, view new products and equipment. See product demonstrations by our friendly team who are happy to give help and advice. |
|
 |
FULL !! FULL!!! SUNDAY 18TH MARCH Doubletree by Hilton NORTH – NEWBURY – RG20 8XY |
OPEN DAYFree entry and open to all, special offers and discounts available on the day. We bring our showroom to you, view new products and equipment. See product demonstrations by our friendly team who are happy to give help and advice. |
|
 |
Saturday 15th September – Heathrow Premier Inn , Bath Rd, 15 Bath Rd, Heathrow, Longford, Hounslow TW6 2AB
|
 |
Saturday 13th October – Manchester Premier Inn Trafford Centre West – Old Park Ln, Stretford, Manchester M17 8PG |
|---|---|
| TO BOOK ONLINE CLICK HERE |
BIOGRAPHY: LAWRENCE DREIFUSS
 |
After graduating from the London Foot Hospital
|

This article will focus on lateral sprain and pain associated with a pes cavus foot structure and a forefoot valgus deformity. Repetitive lateral ankle sprain or lateral knee pain (or even lateral shin splints) is often diagnosed as ‘idiopathic’, closer examination of the biomechanical relevance needs to be pursued. The term ‘idiopathic’ is often used in this area as there seems no reason for the pain occurrence. Pes cavus foot (high arch) structures (Fig. 2) may have a predisposition to lateral ankle sprains and present as a rigid structure and a supinated foot structure.
FIG2
This type of structure will usually exhibit a forefoot valgus deformity
meaning that, ‘the plantar plane of the forefoot remains everted relative to the plantar plane of the rearfoot when the subtalar joint is in neutral.’
This deformity will have an impact on the patient in heel strike, midstance and toe-off phases of gait. The patient who exhibits a pes cavus foot structure will often present with a forefoot valgus (FFVL) greater than 10º and also often exhibit a plantar flexed 1st metatarsal
(Boyd & Bogdan, 1993) – encouraging the foot to strike laterally and eliciting pressure on the lateral aspect of the hip joint. If the forefoot valgus deformity is greater than 10º, the foot will often continue to supinate through the cycle, having a ‘jarring’ effect on the upper structure, putting additional strain on the lateral aspect.

Fig. 3: Use an ICB Protractor to assist in
measurement of Forefoot valgus.
When the foot is supinated it often exerts stress on the peroneals and may cause elongation of the muscles and tendons, thus weakening the retinaculum and lengthening the peroneals, often causing the tendon to sublux off the lateral aspect of the malleolar.
The forefoot valgus deformity (in gait) encourages the foot to invert the foot, propulsion is delayed causing lateral instability and results in tension and tearing of the peroneal muscles, causing inflammation and tenderness, and difficulty walking. Lateral ankle sprains are more common than medial due to the fact that ligaments are weaker on the lateral side.
Hence the lack of lateral stability can be caused by uncompensated or partially compensated rearfoot, a flexible forefoot valgus or osseous forefoot valgus (Boyd & Bogdan, 1993; Hollis et al, 1995; Shapiro et al 1994).
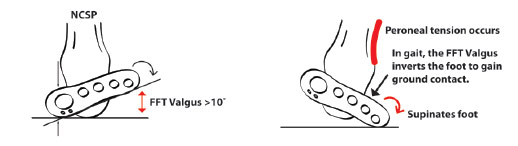
Fig. 4: Effects of Forefoot valgus during gait.
There are also certain biomechanical foot deformities that make some patients more susceptible to inversion sprains, such as, neurological deficits and supinated foot types which exhibit or function with a supinated calcaneus (Valmassy, 1996).
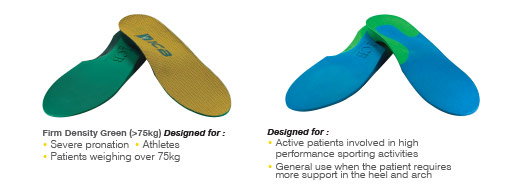
In summary, if a patient presents with lateral hip pain, knee pain, ankle strain or repetitive lateral inversion sprain, always check for a forefoot valgus deformity. If a forefoot valgus if present, add an appropriate size ICB Forefoot Valgus wedge (available in 4° & 6°) to the selected ICB Orthotics using the 3M tape provided. Next, heat mould the ICB Orthotics to the patient’s Neutral Calcaneal Stance Position. Being made from 100% EVA, ICB Orthotics can easily be heated and moulded to suit high arch foot structures.
Prescribing ICB Orthotics.
ICB Heat Moulding Orthotics can be prescribed to assist in the treatment of excessive pronation and supination, and resultant biomechanical conditions. With 5 densities, 5 styles & 11 sizes, there is an ICB Orthotic to suit all footwear styles, patient ages and activity levels.

 PRICES START FROM £18.85
PRICES START FROM £18.85
To enable quick and easy orthotic customisation in the clinic setting, ICB Orthotic Additions are also available, including: Forefoot & Rearfoot wedges, Heel Lifts, Metatarsal domes, medial flanges,
medial arch infills and more.
View the full ICB Orthotic range

Dr.’s REMEDY podiatrist formulated nail care collection has proved popular amongst Podiatrists and Health Care practitioners due to the addition of Tea Tree and the fact that you can use with topical fungus medications which will not make the condition worse.With 37 colours now in the collection we have accumulated the Top 10 sellers in the past 12 months. |
|
|---|---|
 |
 |
|
No.1: Dr.’s REMEDY Mindful Mulberry – |
No.2: Dr.’s REMEDY Peaceful Pink Coral – |
 |
 |
|
No.3: Dr.’s REMEDY Positive Pastel Pink – |
No.4: Dr.’s REMEDY Cozy Cafe – REM6 – A cafe au lait with hints of pinkish grey and a splash of lilac. VIEW |
 |
 |
|
No.5: Dr.’s REMEDY Focus Fuchsia – |
No.6: Dr.’s REMEDY Playful Pink – |
 |
 |
|
No.7: Dr.’s REMEDY Relaxing Rose – |
No.8: Dr.’s REMEDY Clarity Coral – |
 |
 |
|
No.9: Dr.’s REMEDY Remedy Red – |
No.10: Dr.’s REMEDY Balance Brick Red – |
|
|
|
|
|

Management of Achilles tendinopathy in runners-LER
By Howard Kashefsky, DPM
Achilles tendinopathy is a common lower extremity injury in athletes as well as nonathletes. The Achilles tendon is often a site of injury in runners and is the second-most common running-related musculo¬skeletal injury, after medial tibial stress syndrome, with an incidence of 9.1% to 10.9%.
1 The lifetime risk in former elite male distance runners is 52%.
2 Factors that may contribute to Achilles tendinopathy include overuse, systemic disease, older age, sex, body composition, and biomechanics.
3 Elevated biomechanical load has been shown to cause both microscopic and macroscopic failures.4-6
1. Lopes AD, Hespanhol Junior LC, Yeung SS, Costa LO. What are the main running-related musculoskeletal injuries? A systematic review. Sports Med 2012;42(10):891-905.
2. Zafar MS, Mahmood A, Maffulli N. Basic science and clinical aspects of Achilles tendinopathy. Sports Med Arthrosc 2009;17(3):190-197.
3. Magnan B, Bondi M, Pierantoni S, Samaila E. The pathogenesis of Achilles tendinopathy: a systematic review. Foot Ankle Surg 2014;20(3):154-159.
4. O’Brien M. Functional anatomy and physiology of tendons. Clin Sports Med 1992;11(3):505-520.

Why Courtin?
A skincare line based on 100% pure Tea Tree oil. Excellent treatment to help many skin problems. Compact and complete series of products.
Courtin has developed a special total skin care and foot care line containing Original Australian Tea Tree oil. The Courtin Tea Tree range includes a wide variety of salon and direct sale products.
What is Tea Tree oil?
Tea Tree oil is produced from the leaves of the Melaleuca Alternifolia by means of a technological process using steam. This process is subject to painstaking quality controls. The result is a purity level of 100%. Since it is a pure and natural product, the colour of the pure oil product can vary from colourless to light yellow.
Tea Tree oil can stimulate the healing of the conditions listed below
• Bacteria, fungi and viruses
• Ingrown nails
• Itching
• Cracked/chapped skin
• Corns
• Inflamed cuticles
• Psoriasis
• Chilblains: toes, feet or hands
• Warts
• Excessive sweating of feet
• Athlete’s foot

Ways to use Tea Tree Oil
Nail Infections – Apply a few drops of Tea Tree oil to the infected area twice per day and allow to penetrate. Can be used on both hands and feet. Place the hands or feet in warm water bath containing approximately 10ml of Courtin Foot Bath and add 1-2 drops of Pure Tea Tree Oil to the bath. After bathing, pat the hands and feet dry and massage with Courtin Hand & Foot Cream. Retreat the infected areas with Pure Tea Tree Oil.
Sprains – Rub Pure Tea Tree Oil directly on the sprain to ease the pain. Thoroughly wash and dry the feet. Apply Courtin Hand & Foot Cream and massage until absorbed. Apply Pure Tea Tree Oil to the affected areas twice per day.
Perspiring feet – Add 5-10 drops of Tea Tree oil to warm water. Take 5 minute foot bath every evening with Courtin Foot Bath. After the foot bath, apply Courtin Hand & Foot Cream and massage until absorbed. Put several drops of Tea Tree Oil in your shoes or apply some Courtin Foot Deo Spray.
General applications for various conditions:
Vaporisation
To purify the air, place a few drops on a handkerchief, sheet or cloth placed on a radiator or in the hanging radiator humidifier.
Foot Bathing
2 – 3 drops of Tea Tree oil in the bath water combined with the Courtin Footbath.
Compresses
Add 2 – 4 drops of Pure Tea Tree Oil to 10 cl. of water mixed with Courtin Footbath. Mix well. Soak the compresses in the Tea Tree oil solution and place them on the site to be treated for several minutes; repeat several times. Adjust the temperature of the water to the ailment being treated.
Massage
For massages, Tea Tree oil must always be mixed with:
■ For the Feet – Courtin Hand & Foot Cream.
When massaging the face, do not exceed a maximum concentration of 3% essential
Courtin treatments with your pedicure
Your pedicure offers various treatments with the wide range of Courtin Tea Tree products. The Courtin treatments not only act preventively but are exceptionally effective for many foot conditions.

Cosmetic Spa Foot Care Treatment – For most of the day, our feet are enclosed in footwear. This treatment with the unique Spa Foot Mask is a real blessing and you can actually feel the energy flowing back into your feet. A cosmetic and nourishing foot treatment providing total relaxation for body and soul.
Foot Mask – For some extra pampering, you can treat your feet with a nourishing foot mask. After a foot peeling, the toenails and cuticles are massaged with nail oil. After that, a foot mask is applied followed by a massage with a specially formulated, nourishing foot cream.
Courtin Foot Care Home Products

100% Pure Tea Tree Oil – The 100% PureTea Tree Oil is made using natural processes and without additives. It is extremely versatile to use and has cell-renewing, pain relieving and soothing effects.

Hand & Foot Cream – This Hand & Foot Cream both cleanses and soothes. In addition to it’s cleansing and soothing properties, it also prevents odours. After cleansing, apply to dry feet and massage until absorbed.

Chapped skin Cream – The perfect cream for feet with highly chapped soles which can lead to cracks and fissures of the soles. With regular use, this cream softens the chapped skin, helps to prevent cracking and stimulates the healing of your feet. also ideal for raw skin on top of the feet. After cleansing apply to dry feet and massage until absorbed.

Foot Bath – For intensive cleansing and reinvigoration of tired feet, use Courtin Foot Bath. Your feet will feel smooth and fresh again. Prevents unpleasant odours. Mix a spoonful of the gel into approximately 4 litres of water. Bathe the feet in water for 5 min.

Nail Oil – Contains extremely nourishing active ingredients. Returns a natural shine to the nails. Apply once per day and massage for several minutes until the oil has been absorbed by the nail.

Ice Gel– For the invigoration of tired, heavily stressed and burning feet or legs. The Ice Gel is directly absorbed through the skin. It prevents unpleasant odours and stimulates the circulation. Massage from the sole of the foot upward toward the thigh.

Foot Deo Spray – The Foot deodorant Spray keeps the feet fresh and any unpleasant odours are neutralised. Spray the Foot Deo on the tops and soles of the feet and rub it in. Don’t forget to apply between the toes.


Congratulations to Joanna and Luke who gave birth to Frankie on 6th November at 2.28am , 5lb 12oz. We are all looking forward to meeting Frankie soon here at DLT.

With Summer now in full swing, the warm weather and longer days brings a season of parties and outdoor activities. With this in mind, our patients’ footwear will have undoubtedly changed – from winter boots and enclosed styles, to sandals and casual ‘slip-ons’. Often these summery footwear styles offer little or no support to the foot. So what can be done to keep patients on track with their treatment regime, and reduce the re-occurence of existing biomechanical conditions or injuries, during the summer months?
WOMEN’S FOOTWEAR
For women, sandals and ballet flat styles of shoes can easily be fitted with ICB High Heel Orthotics. Although, as the name suggests, this orthotic style was originally designed for fitting into high heels, its narrow slimline design makes them ideal for flat (or low) heeled sandals. Each pair of ICB High Heel Orthotics are supplied with velcro dots to hold the orthotics in place inside the sandal.
HIGH HEEL ORTHOTICS
Ideal for fitting into summer sandals and ballet flats.

Tip: Add a 4° ICB Rearfoot Varus Wedge medially on the plantar surface of each orthotic – this will assist in providing additional pronation control.
ICB Rearfoot Wedges
Can be attached to the orthotic when additional rearfoot control is required (more than the 5° inversion built into 2/3 and full length ICB Orthotics). Patients who pronate more than 5° may require additional rearfoot posting to give optimum results. Sizes available: 2° & 4° (2 or 10 pack with double-sided tape).

MENS FOOTWEAR
‘Boat shoes’ and slip-on mocassin styles are popular summer shoes for men. A common problem with these can be that they are often narrow through the shank of the shoe. The ICB Dress Style Orthotic is a good choice for such styles, as the lateral skive (i.e. no lateral border) accommodates for broader feet, and fits much easier to narrow shoe types. The dual density design offers excellent support and comfort for the burliest of blokes.
 Dress Style Orthotics – Ideal for fitting into mens boat shoes and mocassins.
Dress Style Orthotics – Ideal for fitting into mens boat shoes and mocassins.

| A common complaint amongst patient’s who have been prescribed foot orthotics is ‘pain in the arch’. This type of pain can be the result of 4 common issues: 1. Pain can be due calcification (similar to dupuytren’s contracture) or a fibroma in the body of the Plantar Fascia, or a Ganglion cyst may be present. TREATMENT: If there is calcification in the fascia, use manual therapy to break it down.
VIEW VIDEO: 2. Plantar fasciitis pain can be experienced at the attachment to the calcaneus. TREATMENT: Control rearfoot pronation using orthotics with intrinsic rearfoot posting to realign the feet to the Subtalar Joint Neutral Position (STJN). If additional inversion is required to control and achieve STJN, add extra rearfoot wedges (2° or 4°) to provide additional Calcaneal control2.
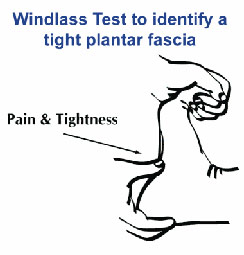
A medial arch infill can also be applied to the orthotic to provide increased arch support. The Plantar fascia may be tight, and during gait (at mid stance to toe-off), compressing into the medial longitudinal arch of the orthotic causing discomfort and pain. To test for a tight fascia use the ‘Windlass Test’ (pictured below).
VIEW DEMO
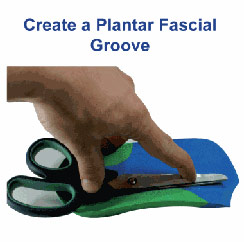
TREATMENT: Create a plantar fascial ‘relief’ or ‘groove’ in the arch of the orthotic using heat or by grinding the orthotic. Place the groove 1cm from the medial edge through the arch contour. 4. The patient may exhibit unilateral excessive pronation as a possible compensation or due to plantar injury.
TREATMENT: Create a plantar fascial ‘relief’ or ‘groove’ in the arch of the orthotic using heat or by grinding the orthotic. Place the groove 1cm from the medial edge through the arch contour
Unilateral arch pain can be associated with a leg length difference3 due to long leg compensatory excessive pronation. If a structural leg length discrepancy is identified, a heel lift will need to applied to the orthotic on the shorter leg.
|
References:
1. FROWEN, P., O’DONNELL, M., LORIMER, D., BURROW, G. (2010) Neales Disorders of the Foot 8th Edition, p130
2. FROWEN, P., O’DONNELL, M., LORIMER, D., BURROW, G. (2010) Neales Disorders of the Foot 8th Edition, p127
3. MICHAUD, T.C. (1997) Foot Orthoses and Other Forms of Conservative Foot Care, Sydney: William & Wilkins, p.114