
![]()
Severs Condition (Calcaneal Apohphysitis) is an inflammation of the growth plate of the bone at the back of the heel (apophysitis of the calcaneus) and occurs during a child’s adolescent years, usually affecting children who are physically active. The point where the inflammation of Severs condition appears is usually localised to the posterior and plantar side of the heel over the calcaneal apophysis – where the Achilles tendon attaches to the back of the calcaneus.
Watch the short video below:

Often young children experience pain in one or both heels whilst engaging in general activities such as running, jumping, or sports such as netball, basketball, football and soccer. Symptoms of Severs Condition include extreme pain when the child places their heel on the ground. This pain is alleviated when the child runs or walks on their toes (i.e. activities that do not exert weight and pressure on the heels). This is because strain is reduced on the epiphyseal plate as the heel is raised off the ground.
The calcaneus takes on a slightly supinated position thus reducing tension on the attachment.
Often full immobilisation is recommended to treat this condition, however, there is no need to plaster the foot or for the child to stop playing sport during the course treatment. That is, unless X-rays show evidence of a fracture in the heel growth plate or epiphyseal plate. (see Fig:1) If a fracture is evident, sporting activities should cease for approximately 6 weeks to allow healing.

This condition usually affects children, between the ages of 8 to 13 years. Severs condition is more common in boys than in girls, and it is uncertain why this appears to be the case. Micheli and Ireland reported on 85 patients, 64% of whom were male1 in their research – however, they did not provide definitive reasons for the skew towards young males.
In one prospective study of injuries among players aged 9-19 years in football academies, 2% of overall football injuries were due to Sever’s Condition; the peak for incidence was in the under-11 age group2. In a study of 85 children, the condition was bilateral in 61%.3
General research opinion agrees that between the ages of 8 and 13 years, children’s bones are still in the growth stage and the growth plates on the skeletal structure have not yet become fused and ossified, which normally occurs by around the age of 17 years4. During the rapid growth surrounding puberty, the apophyseal line appears to be weakened further because of increased fragility of the calcified cartilage.
The combination of growth and poor foot function and mechanics, can cause inflammation and pain at the point where the
tendo-Achilles inserts onto the calcaneus.

Excessive pronation is a major contributing factor when combined together with the child’s growth spurt pattern.
In very severe cases, the growth plate can detach from the calcaneus. Fractures or micro fractures can completely detach the growth plate, pulling it out of position possibly resulting in osteochondritis dissecans.
Neal’s Disorders of the Foot states that, “Repetitive contractions of the muscles of the posterior compartment (gastrocnemius and soleus) may predispose to micro-fractures at the calcaneal epiphyseal plate5.”
Assessment Techniques
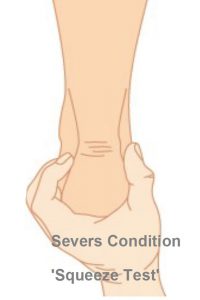
Sever’s condition can be diagnosed based on the child’s medical history and presenting symptoms. A simple and effective test is the calcaneal “squeeze test” which will identify localised pain symptoms and then this will need to be combined with other tests to confirm the diagnosis. Once the squeeze test has been performed practitioners will need to assess for:
* Decreased ankle dorsiflexion.* Abnormal hind foot motion (eg.excessive pronation or supination).* Tight calf muscles* Excessive weight-bearing activities e.g running which will cause deformation of the rearfoot.
Madden and Mellion (1996) noted an means of assessment could be to require the patient to stand on their tip toes, raising and lowering, and gauge whether there was an exacerbation of symptoms6.

View kids Orthotics
Treatment
Orthotic therapy is an excellent treatment regime7 as it realigns the biomechanical structure whilst controlling excessive pronation of the rearfoot.
Stabilising the calcaneus and its growth plate by restricting or limiting excessive pronation can prevent long-term injury and discomfort.
The use of bilateral heel lift of approximately 4mm is recommended in combination with orthotics for short term relief. Removal of the heel lifts, after an initial 2 week acute pain period is recommended, however if additional support and control is required sports strapping using a low dye taping technique can be useful.

Deep tissue massage of the calf muscle (in combination with orthotic therapy), is also a successful mode of treatment. Stretching the calf muscles is however not recommended whilst inflammation is still present, as this may cause further tearing at the attachment. Stretching and deep tissue massage may be in part, prophylactic in the maintenance of the condition.