
![]()
A common complaint amongst patient’s who have been prescribed foot orthotics is ‘pain in the arch’.
This type of pain can be the result of 4 common issues:
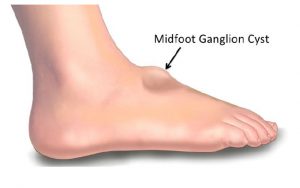
1) Pain can be due calcification (similar to dupuytren’s contracture) or a fibroma in the body of the Plantar Fascia, or a Ganglion cyst may be present. Dupuytren’s contracture in the fascia of the foot is called Ledderhose disease, or plantar fascial fibromatosis, and is sometimes associated with plantar fasciitis.

A ganglion cyst is a tumor or swelling on top of a joint or the covering of a tendon (tissue that connects muscle to bone). Ganglion cysts are among the most common benign soft-tissue masses. Although they most often occur on the wrist, they also frequently develop on the foot usually on the top, but can also occur on the plantar surface. Ganglion cysts vary in size, may get smaller and larger and may even disappear completely, only to return at another time. The exact cause of ganglion cysts is un-known, they may arise from trauma whether a single event or repetitive microtrauma.
TREATMENT: If there is calcification in the fascia, use manual therapy to break it down. For a fibroma or Ganglion cyst, a deflection will need to be heated into the orthotic using a deflective device such as a spoon, to accommodate and relieve any pressure from this area.
Watch this video on youtube on how to use heat to make deflection on an ICB Orthotic.


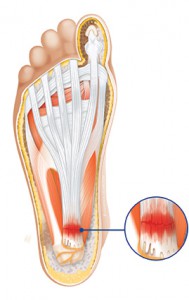
2) Plantar fasciitis pain can be experienced at the attachment to the calcaneus. It is also refered to as Plantar Fasciosis a degenerative syndrome of the plantar fascia resulting from repeated trauma at its origin on the calcaneus1.
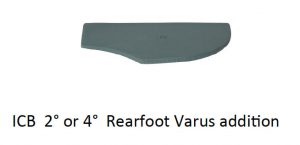
TREATMENT: Control rearfoot pronation using orthotics with intrinsic rearfoot posting to realign the feet to the Subtalar Joint Neutral Position (STJN).
If additional inversion is required to control and achieve STJN, add extra rearfoot wedges (2° or 4°) to provide additional Calcaneal control2.

A medial arch infill can also be applied to the orthotic to provide increased arch support.

3) The Plantar fascia may be tight, and during gait (at mid stance to toe-off), compressing into the medial longitudinal arch of the orthotic causing discomfort and pain. To test for a tight fascia use the ‘Windlass Test’ (pictured below).

TREATMENT: Create a plantar fascial ‘relief’ or ‘groove’ in the arch of the orthotic using heat or by grinding the orthotic. Place the groove 1 cm from the medial edge through the arch contour. Watch video here.

4) The patient may exhibit unilateral excessive pronation as a possible compensation or due to plantar injury.
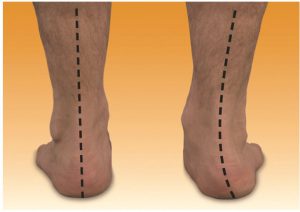
TREATMENT: Unilateral arch pain can be associated with a leg length difference3 due to long leg compensatory excessive pronation. If a structural leg length discrepancy is identified, a heel lift will need to applied to the orthotic on the shorter leg.

SAVE 10% OFF ICB PRODUCTS WITH DISCOUNT CODE: 02ICB10 Offer online only!
References:
1. CORNWALL MW. MCPOIL TG. Plantar Fasciitis: Etiolo-gy and Treatment. J Orthop Sports Phys Therapy 1999;29:756-76.
2. FROWEN, P., O’DONNELL, M., LORIMER, D., BUR-ROW, G. (2010) Neales Disorders of the Foot 8th Edition, p127
3. MICHAUD, T.C. (1997) Foot Orthoses and Other Forms of Conservative Foot Care, Sydney: William & Wilkins, p.114